Year one of the EU HTA Regulation belonged to oncology drugs and ATMPs. Year two opens a more structurally interesting front: the HTA Coordination Group's horizon-scanning report identifies 15 high-risk medical device categories potentially eligible for Joint Clinical Assessment, making 2026 the first year devices meaningfully enter the EU-level process.[1] A qualitative study of HTA bodies' early implementation experience for high-risk devices, published this spring in Value in Health, documents what insiders already suspected: assessment bodies are navigating capacity constraints and genuine uncertainty about how device evidence should be judged within a framework built for medicines.[2]
Practical caveat: this is an HTA methods interpretation, not advice for any specific device JCA. Eligibility, timing, and evidentiary expectations should be checked against current EU HTA Coordination Group outputs and national procedures before dossier planning.
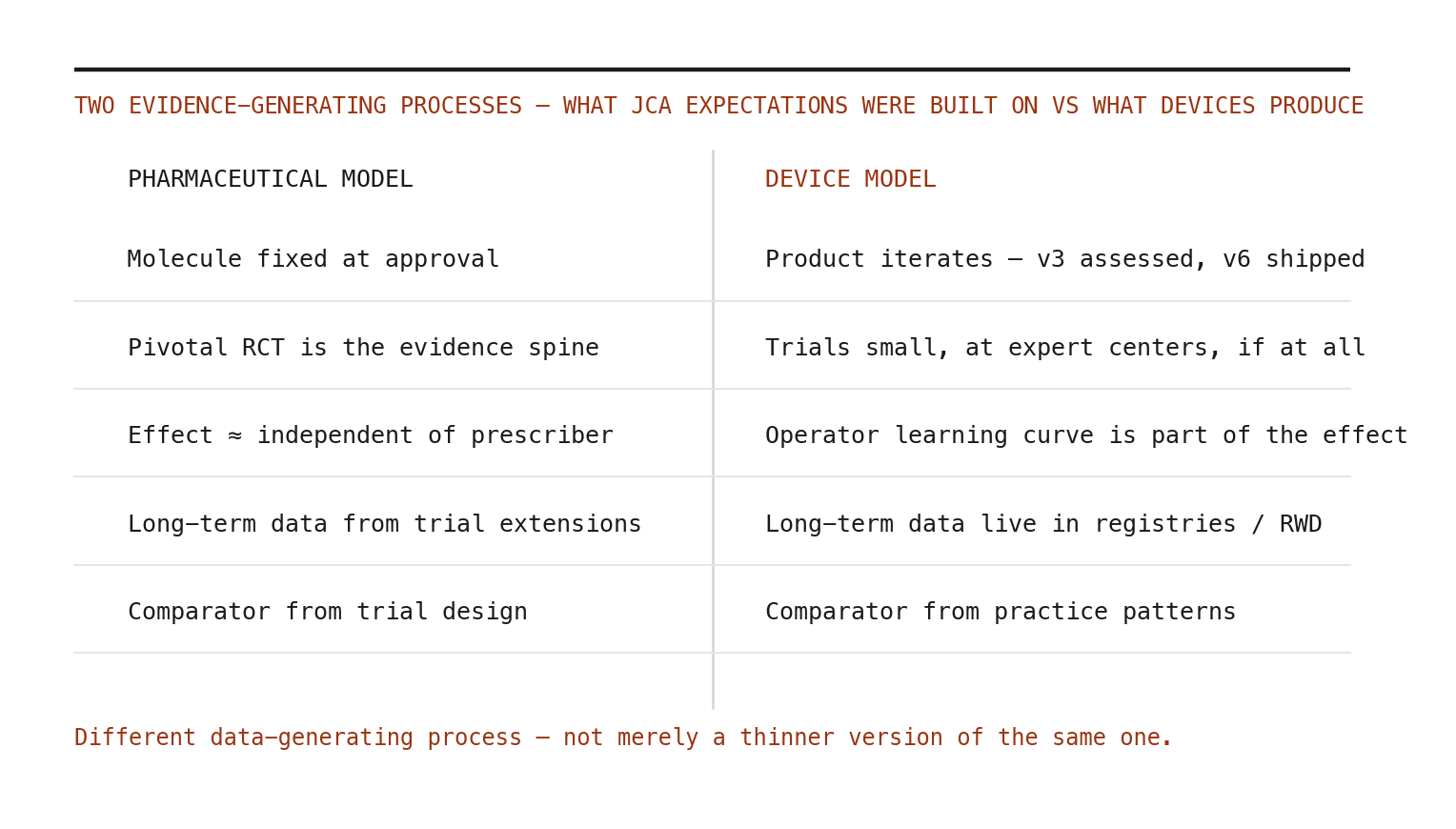
That framework mismatch deserves more attention than it is getting, because it is not a matter of devices having "weaker" evidence. It is a different data-generating process — and pretending otherwise produces assessments that are rigorous in form and uninformative in substance.
Why device evidence is structurally different
Three features, none of them fixable by demanding more RCTs.
Iteration outpaces evaluation. A device assessed at version 3 may be at version 6 by the time the assessment publishes. The pharmaceutical assumption — molecule fixed, evidence accumulates around it — simply does not hold. An assessment regime that cannot handle versioning will perpetually evaluate products that no longer exist.
The operator is part of the intervention. Outcomes for implantables and surgical devices carry learning-curve effects: the same device yields different results in its hundredth versus its thousandth deployment at a center. Trials run at expert centers systematically overestimate real-world effectiveness — not as bias in the pejorative sense, but as a transportability problem baked into the technology class.
Follow-up lives in registries. Long-term device performance — the thing payers and patients actually care about — has historically come from implant registries and routinely collected data, not extended trial follow-up. The best evidence on a hip implant's ten-year survivorship is registry evidence, full stop.
Notice what those three features have in common: every one of them is a real-world evidence problem. Versioned exposure definitions, provider-level effect modification, registry-based long-term outcomes — this is RWE's home turf, the methods territory pharmacoepidemiology and HSR have spent two decades professionalizing.
The opportunity, and the failure mode
The opportunity: device JCAs could become the venue where registry-grade RWE gets treated as primary evidence rather than supplementary garnish — because for this technology class there is frequently no credible alternative. Done well, that precedent then back-propagates to medicines, where regulators and HTA bodies have been inching toward RWE acceptance for years.
The failure mode is equally clear, and the early qualitative findings hint at it: assessors trained on pharmaceutical dossiers apply pivotal-trial expectations to a technology class that cannot meet them, conclude "insufficient evidence" at scale, and the JCA becomes a stamp that says we looked, and the evidence was not shaped like a drug trial.[2] Strictly true. Decisionally useless. And corrosive to the regulation's legitimacy with the device industry from day one.
What would competence look like
For manufacturers: invest now in registry partnerships, pre-specified protocols for observational comparisons (the target trial discipline applies to devices too — with the device version and operator experience as explicit protocol elements), and transparent provenance for routinely collected data. For methodologists: the device-JCA methods playbook — versioning, learning curves, registry quality criteria — is genuinely unwritten, which makes it one of the highest-leverage publication targets in HTA right now. For assessment bodies: borrow the lesson medicines took a decade to learn — the question is never "is this evidence perfect," it is "is this evidence adequate for this decision, with uncertainties named and priced."
Devices entering the JCA is a stress test of whether Europe's new assessment machinery can flex to fit the evidence that actually exists. Watch it closely. The answer will tell you a great deal about how the next decade of RWE acceptance goes — for everything.