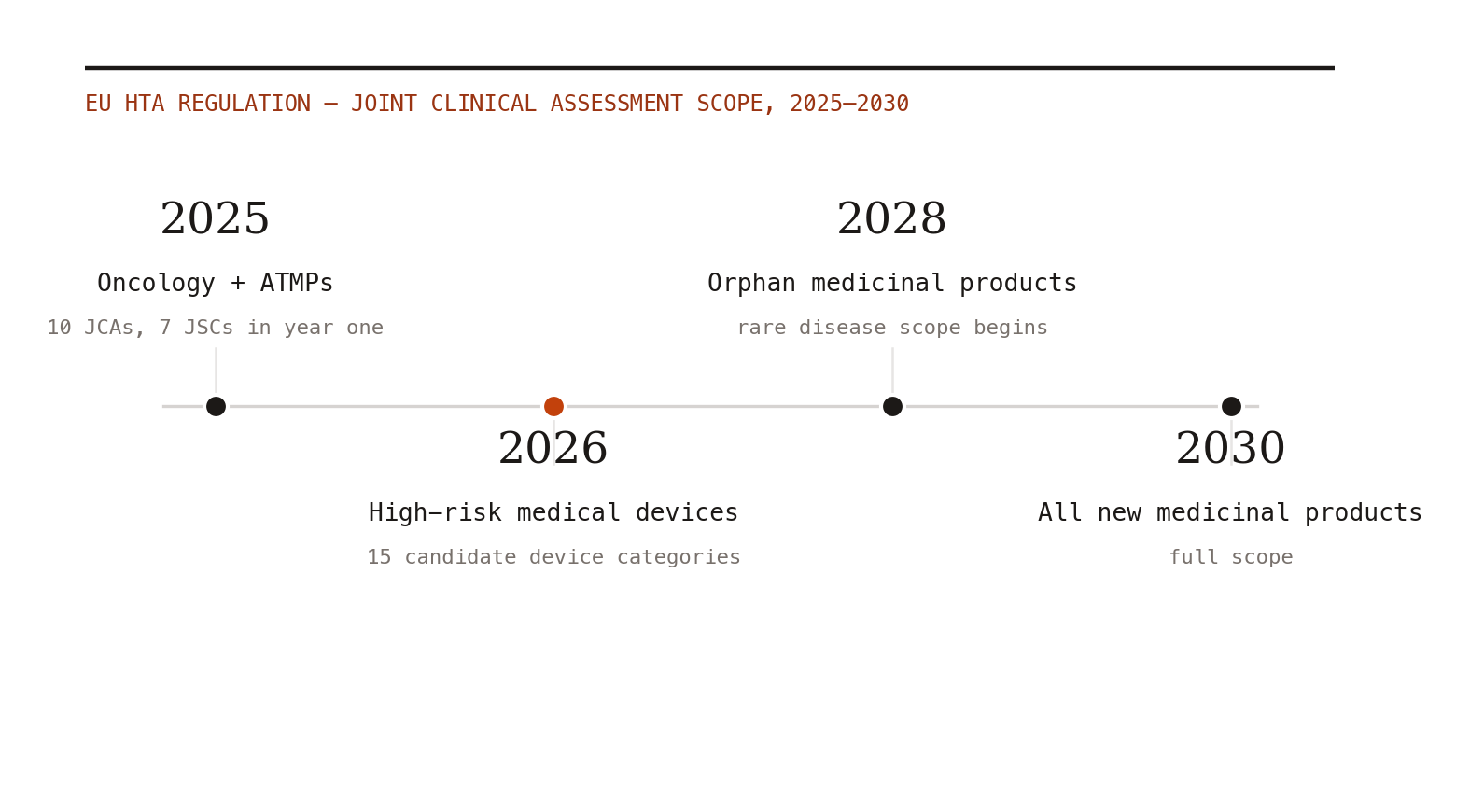
The EU Health Technology Assessment Regulation went operational on January 12, 2025, and the scorecard for year one is now public: ten Joint Clinical Assessments (JCAs) and seven Joint Scientific Consultations (JSCs), concentrated in the launch scope of oncology medicines and advanced therapy medicinal products.[1,2] For a process that skeptics predicted would collapse under its own consensus requirements, "it ran" is a genuine result. But the texture of how it ran is where evidence teams should be paying attention.
Practical caveat: this is a methods-and-market-access read of public JCA materials, not submission or legal advice. Teams should verify current Coordination Group guidance, national implementation rules, and product-specific scoping documents before using it for a live dossier.
The headline finding: PICOs breed
The JCA process builds its evidence requirements from PICO frames (population, intervention, comparator, outcomes) consolidated across 27 member states. In theory, consolidation produces a manageable set. In practice, year one showed that PICO requests multiply wherever treatment recommendations, standard-of-care definitions, and off-label usage diverge across countries — which is to say, nearly everywhere that matters commercially.[1] Rapidly evolving treatment landscapes (exactly the oncology indications in scope) make it worse: the comparator that was standard when you designed your trial may be one of several by the time your PICO set lands.
The resource implication is not subtle. Each marginal PICO can mean another indirect comparison, another subgroup workup, another evidence synthesis — performed on JCA timelines, which do not care about your team's capacity. ICON's first-year review flags exactly this: unforeseen PICOs are resource-intensive to cover, and the uncertainty is structural, not transitional.[1]
What is changing in response
The process is not static. Refinements heading into 2026 aim to involve individual clinical experts and patients earlier, improving transparency and the clinical grounding of assessments.[1] This is the right direction — many year-one PICO surprises were, at root, failures to see a member state's clinical reality early enough.
Meanwhile the scope expands. The HTA Coordination Group's horizon-scanning work identifies 15 high-risk medical device categories potentially eligible for joint assessment in 2026 — the first year devices meaningfully enter the EU-level process.[3] Anyone who has worked device evidence knows the JCA's trial-centric instincts will meet a very different evidence ecosystem there (more on that in a separate brief). Orphan medicinal products enter in January 2028; all new medicinal products by 2030.[2]
The uncomfortable structural truth
A JCA does not replace national appraisal — pricing and reimbursement decisions remain stubbornly national, and member states can still layer their own analyses on top. The Office of Health Economics' framing of "one Europe, one assessment?" keeps the question mark for good reason.[4] What the JCA actually centralizes, so far, is the clinical evidence review — which means manufacturers now face a consolidated, high-stakes, deadline-driven evidence gauntlet in addition to the national mosaic, not instead of it. That may improve over time. Year one does not yet show it.
What I would do differently because of year one
Three practical moves. First, run PICO-anticipation as a formal exercise 18-24 months before expected JCA scoping — map member-state guidelines, off-label patterns, and pipeline competitors, and pre-specify which indirect comparisons you could stand up quickly. Second, treat the JSC as load-bearing: seven happened in year one, and early scientific consultation is the only sanctioned channel for reducing PICO surprise. Third, position your real-world evidence capability as the PICO shock absorber — when a comparator you never trialed against shows up in the consolidated frame, a well-governed external-control or comparative-effectiveness analysis is often the only bridge available on the clock you are given. That is an RWE jobs program hiding inside a regulatory process, if your data and methods are credible enough to take the work.
The JCA's first year proved the machine turns on. Year two tests whether evidence teams can feed it without burning out.