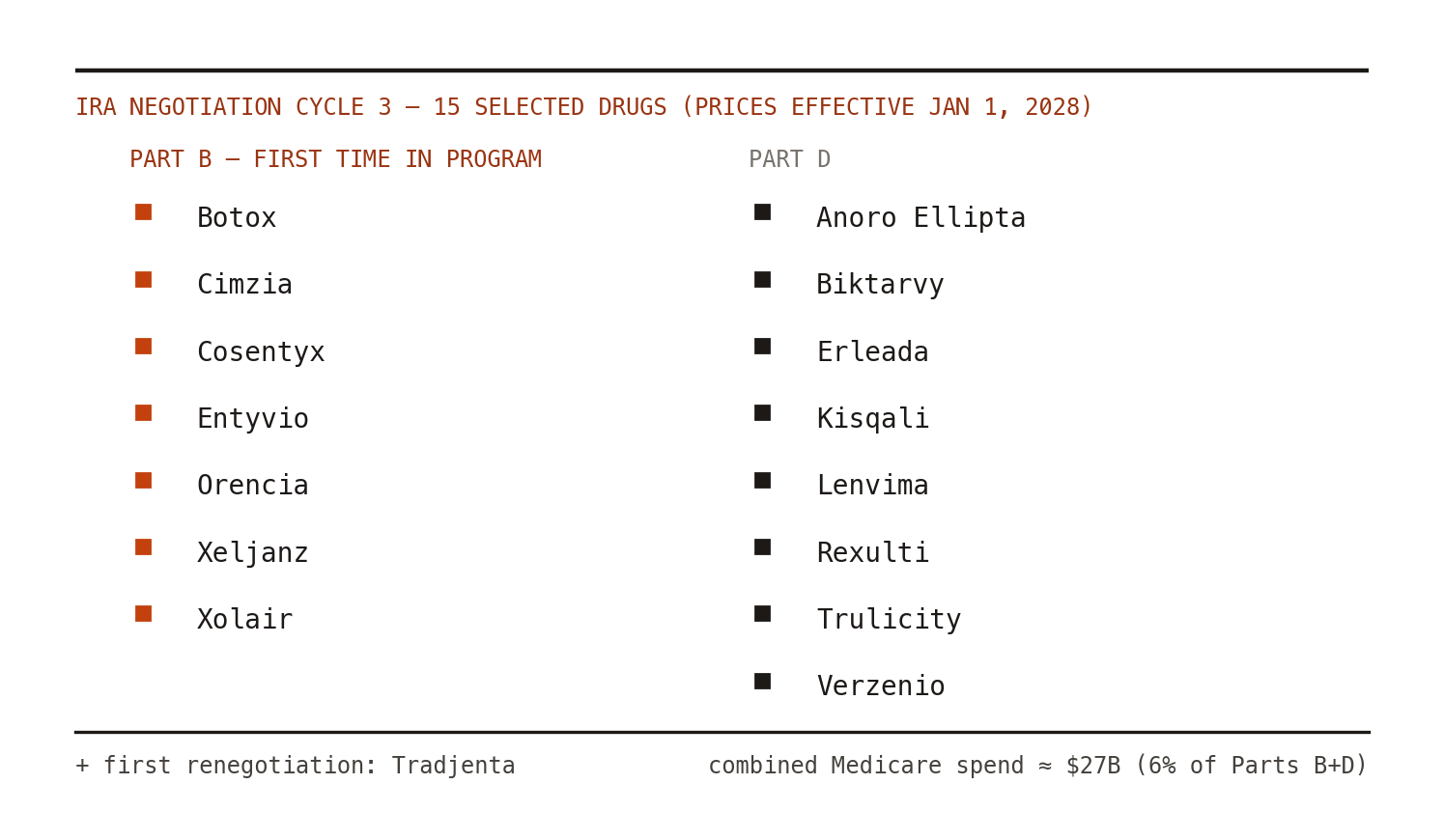
The Inflation Reduction Act's drug price negotiation program stopped being solely a Part D story this winter. On January 27, 2026, CMS announced the 15 drugs selected for the third negotiation cycle, describing the list as drugs "payable under Medicare Part B and/or covered under Medicare Part D" and emphasizing that Part B drugs entered the program for the first time.[1,2] That wording matters: the official CMS materials do not label every selected product by a single benefit category. The clean claim is that cycle three brings Part B-payable drugs into the negotiation perimeter alongside Part D drugs. CMS also selected its first renegotiation: Tradjenta, back for a second pass.[2]
The scale is familiar by now but still worth stating plainly: the selected drugs account for about $27 billion in Medicare spending — roughly 6% of combined Part B and Part D expenditures — used by about 1.8 million beneficiaries in the November 2024 to October 2025 window.[2] CMS announced on March 13, 2026 that the companies manufacturing all 15 selected drugs chose to participate; the statutory agreement deadline was February 28 and submissions from participating companies and the public were due March 1.[3] Negotiations run through 2026; maximum fair prices take effect January 1, 2028.[1]
Practical caveat: this is a policy-methods interpretation of public CMS materials, not legal or regulatory advice. Teams making pricing, contracting, or submission decisions should verify current CMS guidance, drug-specific materials, and their own benefit-channel facts before acting.
Why Part B is a different animal
Part D negotiation, whatever you think of it, operates in a familiar channel: plans, formularies, pharmacy benefit design. Part B is structurally different in three ways that matter for evidence people.
Buy-and-bill economics. Where a selected product is paid through Part B, providers purchase the drug and are reimbursed at average sales price plus an add-on. A negotiated maximum fair price can propagate through provider margins, not just beneficiary cost-sharing — which means utilization responses may run through prescriber incentives, a much messier behavioral system than a formulary tier change. If you model a Part B product as a simple unit-cost substitution, you are doing it wrong.
Biosimilar and competitor interplay. Several selected products sit in categories with biosimilar entrants or close therapeutic substitutes. The negotiation program's interaction with biosimilar uptake — does a negotiated originator price accelerate or strangle biosimilar competition? — is one of the genuinely open empirical questions of the decade, and cycle three gives researchers another setting to study it.[4,5]
Indication breadth. Several selected products span multiple clinical uses. Negotiated prices attach to selected drugs, but CMS considers clinical benefit, therapeutic alternatives, and specific populations in ways that can be indication-sensitive.[5] Expect manufacturer submissions to lean hard on comparative effectiveness across uses, and expect real-world evidence to carry weight where head-to-head trials are absent. If you have spent years arguing your RWE was "decision-grade," CMS negotiation is now one of the decisions.
The renegotiation precedent
Tradjenta's return matters more than its market size. CMS's public explanation of renegotiation is narrower than "all new evidence is automatically in scope": a previously selected drug can become renegotiation-eligible after a change in monopoly status, a new indication, or a material change in statutory negotiation factors.[5] That still converts post-negotiation evidence generation from a nice-to-have into a strategic asset. The portfolio question for HEOR teams: what evidence, generated in the next three years, could credibly affect a future renegotiation factor? Build that plan now, not in the data-submission panic window.
The bottom line
Three cycles in, negotiation is no longer an event — it is an operating condition. The teams treating each cycle as a fire drill are burning out their best people; the teams treating it as a permanent evidence function are getting better at it each round. And with Part B in scope, the evidence questions finally got hard enough to be interesting.