If you have attended enough ISPOR meetings, you can date them by their AI discourse the way geologists date rock strata. 2023: "Will ChatGPT replace the systematic review?" 2024: nervous workshops. 2025: pilot results. ISPOR 2026 in Philadelphia — May 17-20, 4,500+ attendees at the Pennsylvania Convention Center — was the year the question quietly flipped from whether to how do we prove this thing is right?[1,2]
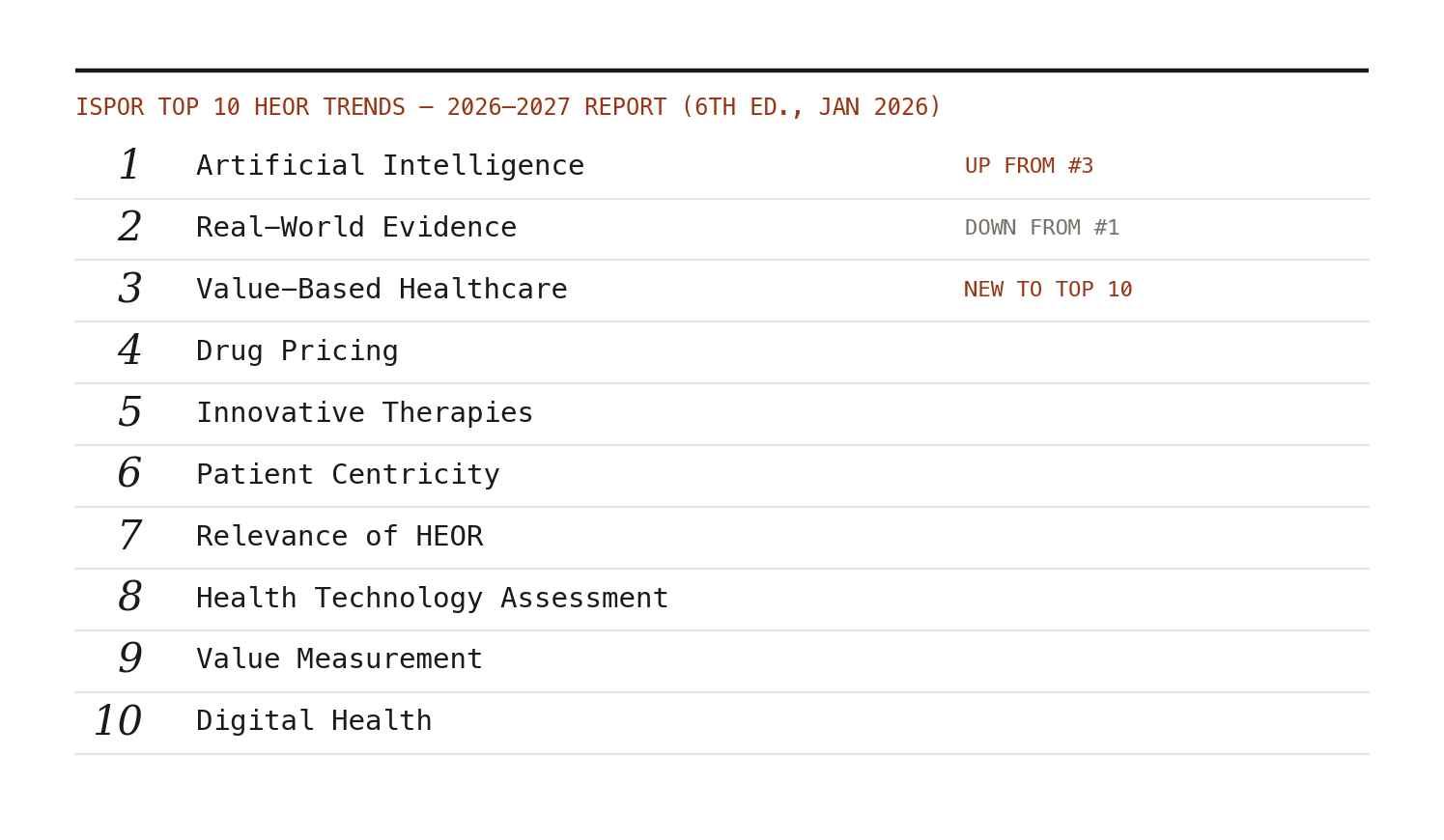
That flip is now official ISPOR doctrine. The society's 2026-2027 Top 10 HEOR Trends report, its sixth edition, put artificial intelligence at #1 for the first time, displacing real-world evidence to #2 after years on top. CEO Rob Abbott's framing was telling: AI is "now embedded across the evidence lifecycle," and the work ahead is "strong governance, transparency and human oversight."[3] Embedded. Not emerging, not promising — embedded.
What the floor actually sounded like
The conference recaps converge on the same observation: sessions on AI were overwhelmingly practical.[2] Organizations presented AI deployed in literature screening, protocol drafting, data abstraction, economic model construction, and HTA dossier preparation — with the interesting arguments happening one level down, at validation strategy, audit trails, and human sign-off points.
This matches what I am seeing inside organizations. Nobody senior is asking "should we use AI?" anymore. They are asking three harder questions. First, which steps tolerate automation — screening tolerates it well, judgment calls about clinical relevance less so. Second, what does validation even mean when the comparator (dual human review) has its own well-documented error rate. Third, who owns the mistake when an AI-assisted model feeds a payer submission.
These are governance questions wearing methods costumes, and HEOR as a field is better equipped for them than we give ourselves credit for. We have spent thirty years building frameworks for "is this evidence good enough for this decision?" Pointing that machinery at AI outputs is not a revolution. It is a Tuesday.
The other four themes deserved more attention
The AI noise crowded out quieter signals worth your time. Global RWE expansion was everywhere — with China's real-world data ambitions drawing real attention alongside real skepticism about governance and comparability in Western HTA settings.[2] Patient-centered value assessment moved from aspiration toward implementation, particularly in oncology and rare disease. Regional HTA divergence got franker treatment than usual: the polite fiction of a "global evidence strategy" is increasingly hard to sustain when US, EU, and Asia-Pacific expectations are actively diverging. And pricing policy — IRA negotiation, MFN deals, international reference pricing — ran underneath everything, because evidence generation and price are no longer separable conversations.[2]
The meta-takeaway from Blue Matter's recap is the one I would underline: evidence, technology, policy, and access are "increasingly interconnected," and HEOR is being treated as a strategic capability rather than a reimbursement support function.[2] That is the most flattering thing anyone has said about this field in a decade. It is also a warning — strategic capabilities get strategic scrutiny.
What to do with this
If you lead an evidence function: your AI story for the next 12 months should be a validation story. The teams that impressed in Philadelphia weren't the ones with the flashiest demos; they were the ones who could show their error rates against a defensible reference standard. If you are a student or early-career researcher: the meeting's real lesson is that methods rigor did not get less valuable — it became the scarce input. Someone has to check the machine, and that someone needs to know what a well-designed study looks like. (That, not prompt engineering, is the durable skill.)
ISPOR 2027 will be in San Diego. I am betting the strata will read: "show me your audit."