Let me state my bias up front: I think Americans pay irrational prices for drugs, I think international reference pricing is a legitimate policy instrument, and I think some of the MFN deals may genuinely help patients. None of that changes the professional complaint I am about to make, which is that you cannot evaluate a policy whose terms you cannot see.
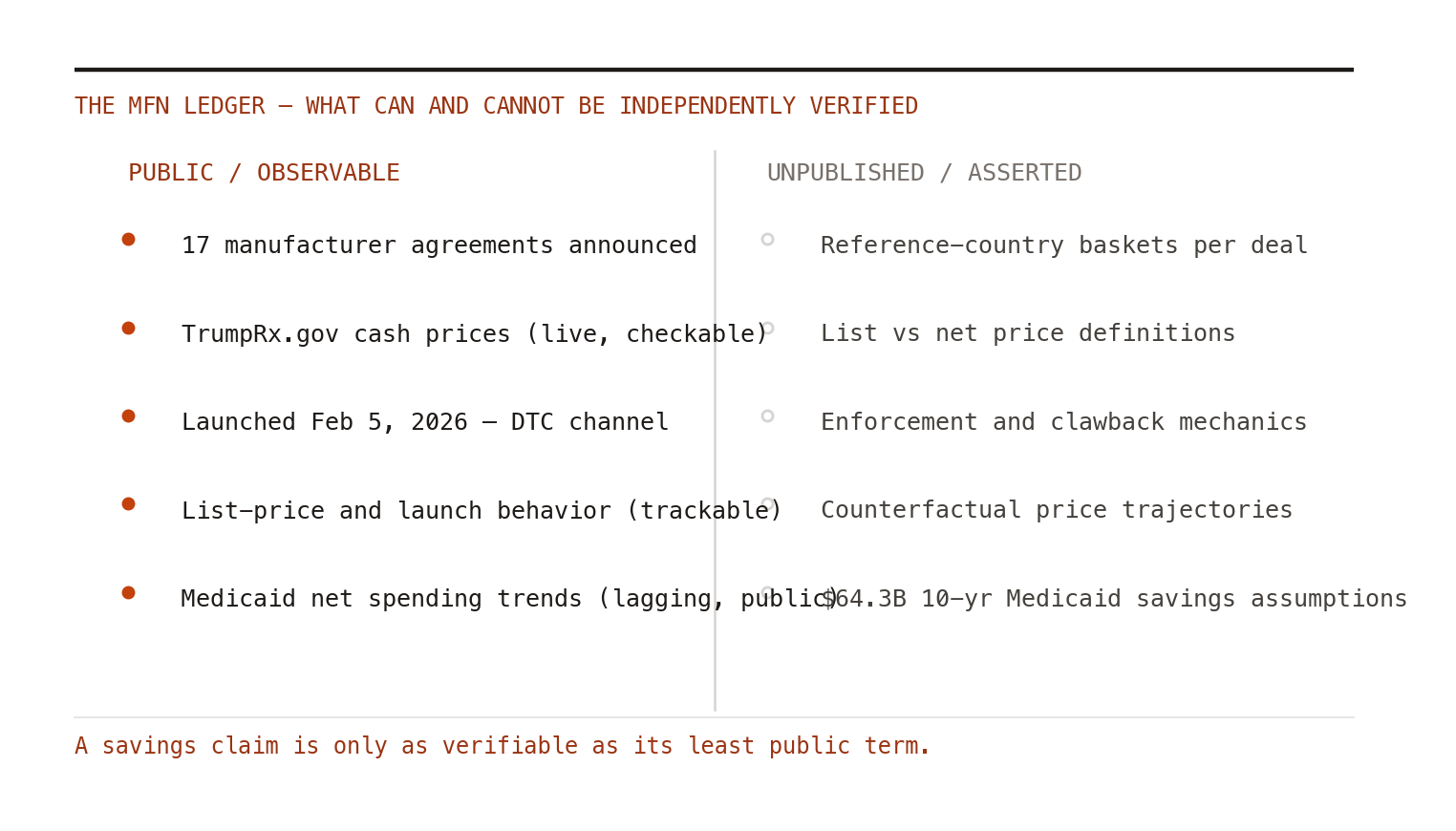
Here is what is publicly claimed. The administration has reached voluntary most-favored-nation pricing agreements with 17 of the largest pharmaceutical manufacturers — by its accounting, 86% of the branded drug market — with Regeneron announced as the seventeenth in late April 2026.[1] TrumpRx.gov, the direct-to-consumer discount channel, launched February 5, 2026, with projected savings of roughly $3,000 per year for uninsured GLP-1 users and $6,000+ for couples pursuing IVF.[2,3] The Council of Economic Advisers' May 2026 report projects $64.3 billion in federal and state Medicaid savings over ten years from MFN-priced drugs.[2]
Some of this is probably real. Cash-pay discounts on GLP-1s, in particular, are observable — you can go to the website and see a price. Good. That part of the program is, to its credit, the most transparent drug pricing intervention in years.
The verification gap
The rest is murkier, and I am far from the only one saying so. STAT's reporting in late May described the deals as clouded by secrecy, with key terms — reference country baskets, list-versus-net price definitions, enforcement and clawback mechanics, timelines — unpublished.[4] Axios reported in February that pressure was already building over what the early Pfizer and Lilly deals actually committed anyone to.[5]
This matters because every savings estimate is exquisitely sensitive to those unpublished terms. "MFN price" against which countries' prices? Gross or net of confidential rebates — the same confidential rebates that make European net prices themselves unobservable? Savings relative to what counterfactual price trajectory? A ten-year, $64.3 billion projection built on assumptions we cannot inspect is not a finding; it is a press release with a confidence interval of vibes.
The bullshit asymmetry principle applies: producing an unverifiable savings claim takes a fact sheet; refuting one takes a research program. Our field is the research program.
What health economists should actually do
Three things, none of them partisan.
Demand the denominators. Every published evaluation of MFN deals should begin by listing the terms that would be needed to verify the claim, and flagging which are public. Normalizing that discipline — a "verifiability table" alongside every budget-impact estimate — is squarely within HEOR's competence and temperament.
Instrument the observable channels. TrumpRx prices, Medicaid net spending, launch sequencing, and list-price behavior are all measurable. The natural experiments are running right now. If MFN pricing causes manufacturers to raise ex-US launch prices or delay ex-US launches — the classic predicted distortion — that will show up in data we can get. Someone should be pre-registering those analyses today, before the outcomes are known and the motivated reasoning begins on both sides.
Refuse the false binary. It is entirely consistent to believe US drug prices need fixing and that this particular mechanism deserves rigorous, adversarial evaluation. The worst outcome for the field is sorting into teams — cheerleaders who accept the savings claims and cynics who dismiss the whole enterprise — when the professionally correct position is the boring one: show us the terms, and we will tell you what they are worth.
Reference pricing imports other countries' price outcomes without importing the assessment processes that produced them. Whether that is clever arbitrage or incoherent freeloading is a genuinely interesting question. It would be nice to be allowed to answer it.