Background. Target trial emulation (TTE) has won the framing war in real-world causal inference — and victory has produced a familiar pathology: the label now appears on studies whose data could never have supported the trial being "emulated." Writing a beautiful protocol is necessary; it has never been sufficient. What the field has lacked is a disciplined account of when electronic health record data can actually realize a given protocol element — and when the emulation is theater.
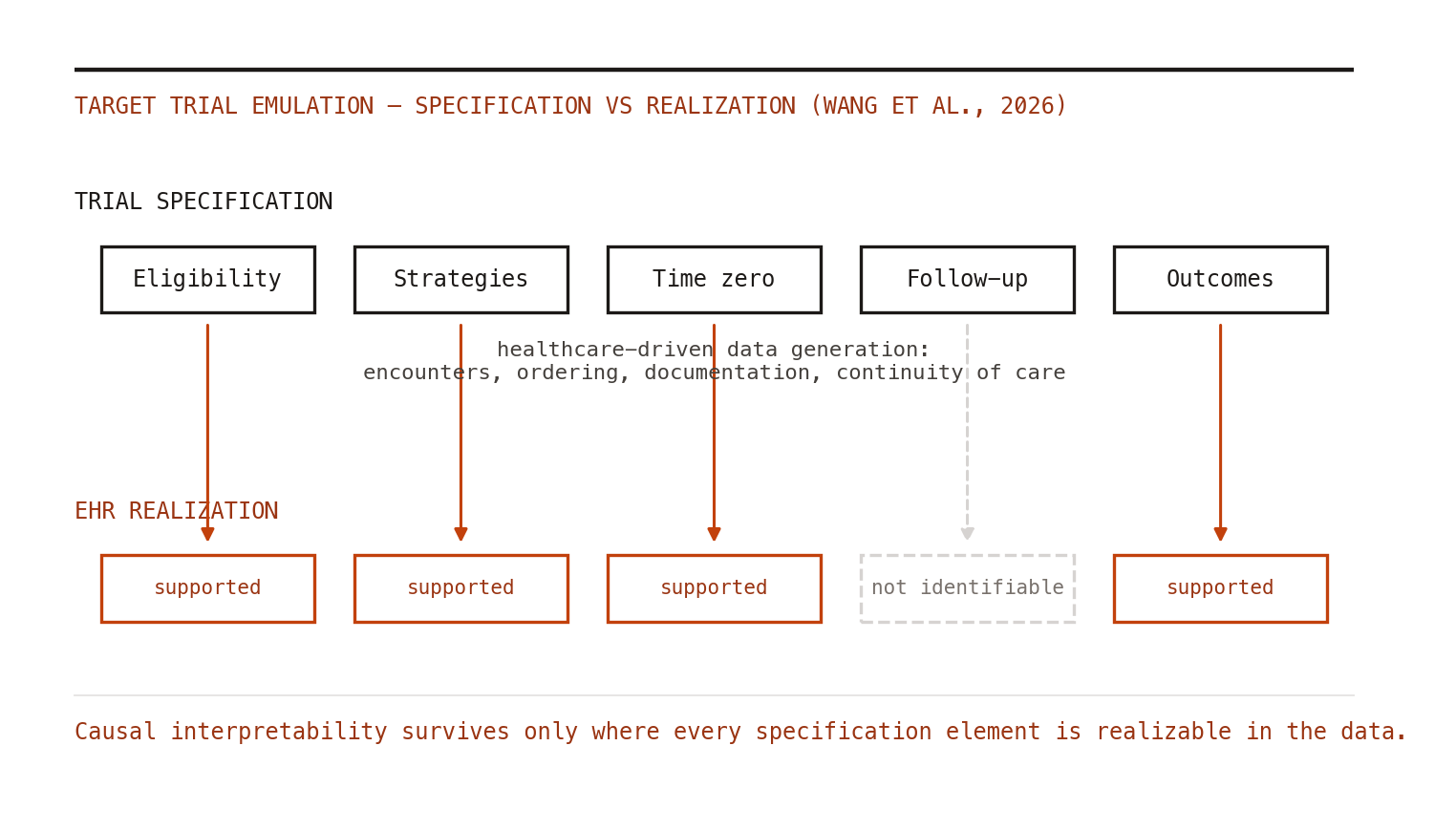
The contribution. Wang, Li, Lin and colleagues, writing in npj Digital Medicine (April 5, 2026), supply exactly that: an operational framework that explicitly separates trial specification from its realization in EHR data.[1] The specification — eligibility, treatment strategies, assignment, time zero, follow-up, outcomes, contrast — is the scientific design act familiar from Hernán and Robins.[2] Realization asks, element by element, whether data generated by the healthcare system's own processes can support that design choice. Their central observation is the one that should be tattooed on every RWD analyst: EHR data are produced by healthcare-driven data generation — encounters happen when patients are sick, labs are ordered when clinicians are suspicious, follow-up exists when care continues — and these mechanisms constrain identifiability in ways no estimator repairs.[1]
Why this matters more than another bias checklist. The framework converts vague worry into specific, checkable questions. Eligibility: can you actually observe the criteria before time zero, or only through diagnostic activity triggered by the outcome process itself? Treatment strategies: does the EHR capture initiation and discontinuation, or only prescriptions written? Follow-up: is "loss to follow-up" ignorable, or is it the healthcare system politely informing you that observation and outcome are entangled? For each element, the answer determines whether an interpretable causal estimate is even on the menu. Some emulations fail at specification-realization alignment, and the correct response is not a fancier weighting scheme — it is a different question, a different data source, or the honesty to not run the study.[1]
Connection to current practice. This lands on fertile ground. The methodological literature has been converging on adjacent worries — a recent Journal of Clinical Epidemiology review catalogs how published "TTE" studies mishandle the alignment of eligibility, treatment assignment, and the start of follow-up,[3] and the NEJM's "potential and pitfalls" essay warned that the label is being applied to designs that emulate nothing in particular.[4] What the new framework adds is an operational dimension: it is not only about aligning times on paper, but about whether the data-generating process permits the alignment at all.
Limitations, honestly stated. This is a conceptual framework, not an empirical validation; its value depends on uptake and on whether reviewers start demanding realization assessments alongside protocols. It is EHR-focused — claims data have related but distinct generation mechanisms (adjudication, enrollment churn, coding incentives) deserving their own treatment. And frameworks do not enforce themselves: the same incentives that produced cargo-cult TTE can produce cargo-cult realization tables.
Bottom line. For practitioners, the immediate move is simple and free: add a realization column to your target trial protocol table. For every protocol element, state the EHR mechanism that generates the relevant data and whether it supports the element's requirements. Where it does not, say so, and say what that costs you. Ten years of TTE adoption taught the field to write protocols. The next five will be about admitting when the data declines to sign them — because the alternative, as ever, is learning it from a regulator's information request instead.